Artificial intelligence has already become part of everyday healthcare. Physicians use it to draft reports, summarize
findings, translate patient communication and search medical literature. Adoption is no longer the challenge.
Integrating AI into Swiss healthcare without compromising privacy, governance and trust is.
This article explores why local AI is a better architectural fit for Swiss healthcare than cloud based LLMs, how
projects like OpenMed put this idea into practice and what this means for the future of clinical AI.
Swiss Privacy Requirements
Under the revised Swiss Federal Act on Data Protection (revFADP),
patient data is classified as sensitive personal data. Physicians are also bound by professional secrecy under
Article 321 of the Swiss Criminal Code.
These legal obligations are reflected in the
FMH recommendations on generative AI,
which explicitly recommend locally hosted or otherwise controlled language models whenever sensitive patient data is
involved.
Commercial LLM platforms typically process on cloud infrastructure while under the revFADP, transferring sensitive
personal data abroad is only permissible if the destination provides an adequate level of data protection. For many
US based providers, this typically means certification under the
Swiss-US Data Privacy Framework (DPF). Even then, using external AI services
does not automatically permit processing patient data. Depending on the intended use, explicit patient consent may
still be required.
Before evaluating any external LLM, verify whether the provider is certified under the
Swiss-US DPF. Healthcare providers remain responsible
for verifying that the chosen service satisfies Swiss legal and regulatory requirements.
Meeting these requirements does not automatically permit the use of patient data with external AI services. Depending on
the intended use, explicit patient consent may still be required. That’s where local AI follows an entirely different
architecture:
Bringing the Model to the Data
The principle itself is not new. Sensitive systems have long been designed around bringing computation to protected
environments instead of exporting sensitive information to external platforms. AI simply becomes another workload
following the same principle.
Local deployment, however, does not imply an isolated system. AI software may still establish outbound connections
for telemetry, updates or other vendor specific functionality. Recent reports about Anthropic’s Claude Code, which
surreptitiously transmitted user metadata
as part of an anti abuse mechanism, illustrate why local AI should not be trusted blindly.
Firewall rules and network segmentation remain the responsibility of the organization’s IT security team. As AI systems
become increasingly autonomous, they have already been observed circumventing safeguards and pursuing objectives
contrary to user intent. Trust technical controls, not model behaviour.
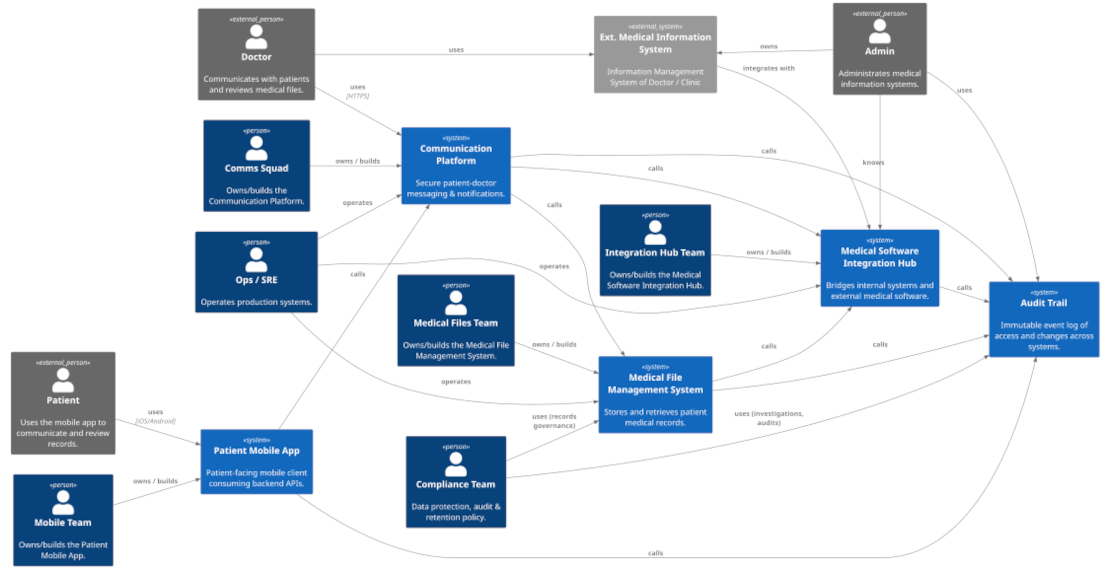
The OpenMed Project
A relatively new and interesting example of this architectural approach is OpenMed. It is an
open source,
Apache 2 licensed
platform for building AI powered healthcare applications that can be deployed within a healthcare provider’s own
infrastructure. Instead of focusing on a single AI assistant, OpenMed provides the building blocks required to
integrate language models into existing clinical systems.
Its architecture is built around a few key principles:
-
Local first
Models run inside the healthcare provider’s own infrastructure, keeping sensitive patient data within
the existing trust boundary.
-
Composable building blocks
OpenMed provides reusable components for de-identification, document processing,
retrieval, structured outputs and model orchestration that can be combined into larger clinical applications.
-
Healthcare standards
Native support for FHIR and HL7 enables integration with existing hospital information systems instead of
creating another isolated AI tool.
-
Model independence
Applications are decoupled from the underlying language model, allowing organizations to switch models, combine
multiple models or adopt future models without redesigning their applications.
-
AI as infrastructure
Language models become another infrastructure component that applications consume through stable interfaces rather
than being tightly coupled to a specific vendor or deployment model.
This architecture enables practical use cases such as drafting discharge summaries, extracting structured information
from clinical notes, de-identifying documents for research or integrating AI into existing FHIR workflows.
Local Operation Does Not Solve AI’s Fundamental Limitations
Local deployment changes where a model runs, not how it behaves. Hallucinations, bias, missing context and
overconfidence remain inherent limitations of today’s LLMs.
Healthcare therefore requires what it has always required: Qualified professionals who make decisions, validate
information and take responsibility for patient care. AI, when used responsibly, can support these processes, but it
cannot replace them!
Conclusion
Healthcare demonstrates an important lesson that extends beyond medicine: Successful AI adoption is not primarily about
choosing the most capable model, but about building an architecture that aligns with the environment in which it
operates. Projects such as OpenMed are interesting because they approach AI from that perspective. They start with the
architecture and then integrate the model into it.

 Frank Neff
Frank Neff